

The trans wave was caused by social influences
The evidence is too strong to ignore


An infographic summarising this article was published in Plain Sight.
The parents writing at Parents with Inconvenient Truths about Trans, like thousands of other parents around the world, believe that their children are being socially influenced towards gender transition. One mother writes:
The first sign that there was something very wrong was when Sinead was 12 and she became unhappy, withdrawn and angry seemingly overnight. She came out as non-binary and then trans when she was thirteen and a half after first self-diagnosing with everything from BPD (borderline personality disorder) to DID (Dissociative Identity Disorder). She was self-harming and had lost all interest in schoolwork or family life. Covid didn’t help and the lockdowns allowed her to spend hours on the internet when she was supposed to be doing online school. I found out later that influencers like Jammie Dodger and Noah Finnce were indoctrinating her into the trans cult and she was also talking to disturbed kids like herself on Discord… I had [also] been witnessing the carry-on of my daughter’s group of friends with all the talk of trans and demi-boys, agender, ace, non-binary and so on… Sinead had been indoctrinated by the internet and to a lesser degree her peers…
It was unthinkable to me that Sinead was ‘trans’. A parent’s first rule in life is to protect their child and that means that the thought of someone slicing off pieces of her healthy body and destroying her health with hormones sickened me. I would sooner volunteer that I sacrifice bits of myself than that she would do this to herself…
Sinead did not agree with her mother’s perspective, and their relationship deteriorated. Sinead’s mother writes that when Sinead “did voluntarily talk to me it was to subject me to angry rants about how she had always been a boy”. But Sinead’s mother held fast to her beliefs. She restricted her daughter’s internet access, spent time rebuilding her relationship with her daughter, and showed her daughter videos that exposed her to different ways of understanding her experience. She encouraged her to engage in healthy activities and interests. Over time, Sinead desisted from her trans identity.
Sinead’s mother writes:
I know that I did the right thing because Sinead told me so. She has thanked me many times and although I was only doing my duty and it was a pleasure to do it, it is still nice to know that she is grateful. I know that I did the right thing because she is happy again. Without even intending it I am now very good friends with Sinead (while still being the parent). I really enjoy her company and I am so grateful that I am getting the opportunity to get to know her again.
Did Sinead’s mother do the right thing? Is it possible that Sinead was influenced into identifying as trans by her peers and the internet, as her mother believes (and, it seems, Sinead now agrees)? Did her mother save her from a lifetime of unnecessary medicalisation? Or was Sinead trying to express her true, innate, immutable gender identity, and did her mother prevent her from becoming her authentic self?
In the past decade, the number of young people seeking medical gender transition has risen dramatically, with devastating health consequences. Understanding the reasons for this rise is crucial to understanding teenagers like Sinead, and how parents and professionals can help them.
There are two main hypotheses that seek to explain the trans wave. The innate hypothesis holds that the trans wave was caused by greater acceptance of gender transition. According to this hypothesis, trans identities have not really become more common in recent years - they have merely become more visible. This hypothesis thus implies that in the past, many people suffered from a suppressed longing to transition. As stigma and barriers to transition have fallen away, innately trans youth have had the freedom to express themselves and find fulfilment, happiness, and contentment by altering their appearance with drugs and surgeries.
The innate hypothesis is rooted in gender identity theory - that is, the belief that everyone has an innate ‘gender identity’. This theory holds that when there is a mismatch between the sex you were born and your gender identity (as male, female, or something else), then that makes you transgender. This mismatch is hypothesised to cause suffering that can only be relieved by medical interventions that reshape your physical appearance to align with your gender identity. According to this theory, because your gender identity is (supposedly) innate and immutable, it cannot be altered by social influences. Thus, no amount of social influence can change whether someone is ‘really’ trans - only whether they reveal to others that they are trans.
In contrast, the social influence hypothesis holds that various social forces have encouraged more people to identify as trans - it’s not just that trans people have become more visible. The social influence hypothesis is based on the theory that identifying as transgender, like most other human behaviour, is influenced by a range of biological, psychological, and social factors.
While gender activists sometimes attempt to paint the social influence hypothesis as a fringe idea, this hypothesis has in fact enjoyed considerable mainstream attention. Respected media outlets and academic journals that have published articles favouring the social influence hypothesis include The Economist, The Times, The Australian, The Atlantic, The New York Times, The Guardian, MedScape, Skeptic magazine, PLOS ONE, the Archives of Sexual Behaviour, Sexuologie, The New Bioethics, and the Journal of Open Inquiry in the Behavioral Sciences.
Numerous researchers and clinicians have argued in favour of the social influence hypothesis. A few of the more prominent of these include:
The National Association of Practicing Psychiatrists (Australia).
Erica Anderson (former president of the United States Professional Association for Transgender Health and a transwoman).
Carol Tavris (social psychologist and Association for Psychological Science Champion of Psychological Science).
David Bell (psychiatrist and former governor of the Tavistock and Portman National Health Service foundation trust).
David Geary (Curators’ Distinguished Professor in the Department of Psychological Sciences, University of Missouri).
James Cantor (clinical psychologist, sex researcher, and Associate Professor at the University of Toronto).
Michael Bailey (professor of psychology at Northwestern University).
Lisa Littman (president and director of the Institute for Comprehensive Gender Dysphoria Research).
Dianna Kenny (former professor of psychology at the University of Sydney).
Celso Arango (former president of the Spanish Society of Psychiatry).
Céline Masson and Caroline Eliacheff (a French clinical psychologist and a child psychiatrist who were joint winners of the Marcelle Blum bursary for the study of female psychology).
Riittakerttu Kaltiala (chief psychiatrist in the department of adolescent psychiatry at Finland’s Tampere University Hospital).
Jonathan Haidt (social psychologist at New York University’s Stern School of Business).
Michael Biggs (associate professor of sociology at the University of Oxford).
The most recent, and authoritative, endorsement of the social influence hypothesis comes from the Cass Review of gender-identity services for children and young people in the UK. This independent review concluded that “societal acceptance... is not an adequate explanation for the overall phenomenon” of the explosion in trans identities. The review instead acknowledges that various “peer and socio-cultural influences” have likely contributed to the trans wave. In an interview with The Guardian, Dr Hilary Cass (the paediatrician who led the review) has stated frankly that there has been “some very dangerous influencing going on”.
The fact that so many respected researchers and clinicians have spoken out in favour of the social influence hypothesis, despite often vicious attacks by gender activists, is a testament to its credibility and importance. While several professional organisations have issued statements disagreeing with the social influence hypothesis (or at least certain forms of it), these statements are influenced by activists and do not necessarily reflect the best evidence or imply a consensus among their members.
The social influence hypothesis offers hope. It implies that trans-identified youth have multiple options for finding happiness. The innate hypothesis, in contrast, implies that these children and adolescents face an inevitable future of either permanent medicalisation (which carries serious health risks), lifelong psychological distress, or both (a common outcome of medical transition). Therefore, it’s worth examining the evidence for both hypotheses carefully, rather than being too quick to dismiss one or the other for political reasons.
Of course, the social influence hypothesis does not imply that people who transition genders should be treated with any less respect and dignity. Nor does it imply that medical transition should be prohibited, at least not for mature adults who are fully informed of the risks. It does, however, suggest that a cautious approach to teaching children about gender, and to medical transition, is warranted.
To more fully understand the social influence hypothesis, it’s worth exploring the range of factors that might cause someone to identify as transgender.
Six reasons to be trans
Most researchers do not appear to believe that trans identities are innate or immune to social influences. The aforementioned Cass Review concluded that “There is broad agreement that gender incongruence is a result of a complex interplay between biological, psychological and social factors”. Similarly, the Endocrine Society describes itself as “a community of 18,000-plus endocrine investigators and clinicians...in more than 100 countries”. The Society writes bluntly in its Scientific Statement on Sex as a Biological Variable in Basic and Clinical Studies:
Although gender is strongly influenced by environmental and cultural forces, it is unknown if the choice to function in society in male, female, or other role(s) is also affected by biological factors.
What then are the biological, social, psychological, and cultural factors that lead to a trans identity? Both research and testimony from trans people themselves point to at least six broad factors, different combinations of which may be at play in any individual case. With the exception of sexual motives, all these factors are mentioned by the Cass Review.
Discomfort with fitting into gender roles and stereotypes
Some children are extremely gender nonconforming, meaning that they prefer to dress, play, and behave in ways that are more typical of the opposite sex. Evidence suggests that gender nonconformity has a significant genetic and/or biological component.
Gender nonconforming children and adolescents are sometimes rejected, bullied, or simply feel that they don’t fit in as well as they should. Unsurprisingly, on average these young people are unhappier than their peers. Some gender nonconforming children wish that they were the other sex, perhaps because they believe this would make others accept them more. Because young children’s understanding of ‘male’ and ‘female’ can sometimes be influenced more by sex stereotypes than by biology, occasionally these children even imagine that they really are the opposite sex. In a few children this combination of factors causes a fixation on becoming the opposite sex which is associated with significant distress (i.e. ‘gender dysphoria’).
Childhood gender nonconformity is often (although not always) associated with being gay or lesbian as an adult, rather than trans. Studies suggest that childhood gender dysphoria typically, but not always, resolves naturally over time (although social transition and puberty blockers appear to disrupt this natural process). However, persistent gender dysphoria, and/or the quest to persuade others to fully accept their gender nonconformity, motivates some people to adopt a trans identity and seek medical transition.
An example of someone who seems to fit the theme of a transition motivated by gender nonconformity is transman Zander Keig, who says:
I transitioned to be a man because I did not fit the stereotype of what it means to be a woman. I was once called a dyke and had a bottle thrown at my head by a passing car. I transitioned because I thought life would be easier for me to live as a man than as a masculine woman—and I was right, because our society’s adherence to rigid gender stereotypes made living my life as I was unbearable.
I wish the message that we should be free to be who we are, had been allowed to win over society. If it had, I might not have felt the need to make the medically risky choice to transition.
Recently, schools, libraries, and other trusted authorities have started to teach children that gender nonconformity is a potential sign of ‘being trans’. This may be one factor contributing to the trans wave.
For individuals suffering distress resulting from gender nonconformity, greater self- and societal acceptance is a potential alternative route to relief.
Sexual motives
Some men acknowledge being sexually aroused by the thought of themselves as women. These men enjoy dressing, acting, and being treated as women during sex or masturbation (and they have documented this interest in copious amounts of porn - links are not safe for work).
Some researchers believe that these sexual interests are related to an underlying sexual orientation, which they call autogynephilia. They also hypothesise that autogynephilic men can, in a sense, fall in love with their image of themselves as female (i.e. their female gender identity). The inability to make this imagined self real causes severe distress (i.e. gender dysphoria). This gender dysphoria can lead to a desire to be treated as female across every aspect of the person’s life, and spur the decision to medically transition.
Just like the love between a romantic couple, autogynephilic desire is not purely sexual, and can persist even after someone’s sex drive fades (e.g. due to the impact of cross-sex hormones). The theory holds that autogynephilia is found in heterosexual and bisexual transwomen (i.e. natal males attracted to women), and that homosexual transwomen (i.e. those attracted to men) have other reasons for transitioning.
While the existence of autogynephilic fantasies is not in serious dispute, various authors have debated whether autogynephilia drives medical transition, and if so how often. In one survey of heterosexual transwomen, 86% reported that they at least sometimes experienced sexual arousal while cross-dressing. However, only 27% reported that their “Concrete sexual fantasies played a role in making the decision to transition”. Interestingly, one study of detransitioners found that 39% of men (and 13% of women) acknowledged that “I had erotic reasons for wanting to transition”.
Possibly, some transwomen may be too ashamed to acknowledge the reasons they transitioned, and self-insight is not always perfect. This makes it hard to verify the proportion of transwomen who transition because of autogynephilia. However, the activist claim that autogynephilia is a “a mere pseudoscientific talking point in anti-transgender propaganda” implies that everyone who says that their transition had a sexual component is mistaken, which seems implausible (and ignores considerable evidence).
While some researchers believe that autogynephilia is probably innate, other writers have suggested that the recent explosion of trans-themed online porn is contributing to the trans wave. To my knowledge, evidence for this connection remains anecdotal.
It’s not uncommon for men to report being aroused by sexual fantasies involving cross-dressing without wanting to medically transition. This suggests that the way that these fantasies are interpreted may be key to whether they trigger a desire for transition. Recent shifts in societal narratives about trans issues may have caused more men to interpret autogynephilic feelings as a sign that they ‘are trans’ and need to medically transition.
An example of someone who appears to have transitioned for at least partly sexual motives is trans author Andrea Long Chu, who famously wrote, “Sissy porn did make me trans”.
For at least some autogynephilic men, finding other ways to channel their sexual desires, without medical intervention, is a potential alternative route to contentment (as is coming to terms with the fact that they can never truly be female).
The belief that transition will alleviate distress
Recently, a new cohort of adolescents have emerged, who identify as trans after a long period of psychological distress. Some are young women who are uncomfortable with their developing bodies, or who have experienced sexual assault. Often these young people have no history of significant gender nonconformity.
Typically, these young people hold a strong belief that medical transition will alleviate their distress, and this motivates their desire to transition.
An example of someone who appears to fit this theme is Noah, a young woman who started identifying as trans as a teenager, and had her breasts surgically removed at age 16. Noah is not gender noncoforming - she acknowledges that, “I have feminine interests and I had feminine interests growing up”. Noah was interviewed by Nelly Bowles on the Witch Trials of JK Rowling podcast:
Nelly: And were you seeing a therapist or a counselor at that time? Like when all of this started.
Noah: I had a lot of mental issues. Maybe that's not the most delicate way to say that, but I was dealing with a lot of mental struggles once puberty began.
Nelly: You mean aside from your issues with gender?
Noah: Yeah, and I couldn't really identify that I had issues with gender. I just had all of these abstract feelings that didn't coalesce into gender dysphoria until I understood what that term meant fully, which was later on in my life. And so I was dealing with very severe anxiety disorder, a depressive disorder, obsessive compulsive disorder and attention deficit hyperactive disorder. And so my mom got me a therapist who I've been with ever since. And when she picked out that therapist, she picked out someone who specialized in anxiety and gender issues and adolescence, which I find interesting to look back on. And I had a psychiatrist as well. And around eighth grade I went into this really severe depressive episode and I ended up telling my psychiatrist that I was debating suicide.
And so everyone decided that we were gonna have to like keep an eye on me. And so I just kept going to therapy and like I said, the core issue which we couldn't figure out was never resolved. And I believe within a year I joined a support group for transgender youths and my therapist helped me identify that a lot of what I had been expressing to her for a really long time could be identified as feelings of gender dysphoria. And after at least a year and a half or two years of those issues being present, she referred me to a gender clinician and talking to my parents was the first big step that was taken.
We identified what I wanted from the gender clinic, which was to go on testosterone and to get top surgery… it had to become very clear that not only was my gender dysphoria spawning all of the other mental issues I was having, but that the solution was medical intervention. And that was seemingly the only thing that could help me because we had tried pretty much every other option at that point.
As both researchers and clinicians have noticed, stories like Noah’s are eerily reminiscent of the ‘repressed memories’ scandal. In the 1980s and early 90s, numerous patients (often young women) came to falsely believe that they had been sexually abused as children.
These patients, like Noah, often presented to therapy with seemingly intractable psychological distress. The 80s and 90s patients saw therapists who specialised in uncovering ‘repressed memories’ - that is, supposed memories of abuse so horrific that they had been hidden from the conscious mind. Over time, through a process of exploration and suggestion, these patients came to truly believe that they had been sexually abused. Sometimes, parents were imprisoned on the basis of these supposedly recovered memories.
Noah, on the other hand, saw a therapist who specialised in gender issues. As Noah tells it, there were no initial signs that her distress had any connection with gender. However, Noah’s therapist appears to have suggested that gender dysphoria (i.e. a repressed trans identity) could be at the heart of her distress, offering her a potential road to self-understanding and recovery.
Over time, through a process of exploration and under the influence of her therapist, a trans support group, and online trans influencer content, Noah came to believe that she was definitely, truly, innately trans. Now that she has taken the drastic step of surgically removing her breasts, this belief would take tremendous courage to let go of, because this would require acknowledging and living with a terrible, life-altering mistake. And acknowledging serious mistakes is something that most people find very hard to do.
While Noah’s therapist appears to have encouraged her belief that transition would relieve her distress (alongside other influences), other adolescents are discovering the same idea outside of therapy (e.g. in the media, on social media, and from friends).
Young people who transition to relieve distress might instead benefit from more effective, and less invasive, treatments for conditions like anxiety and depression.
Peer and online influences
People, especially adolescents, have a powerful drive to belong. This makes us highly susceptible to influence from those around us.
The idea that peer and online influences might play a strong role in some gender transitions was first brought to widespread public attention by Lisa Littman, a physician and researcher at Brown University.
Littman’s curiosity was piqued by the sharp increase in youth seeking treatment at gender clinics. Additionally, both clinicians and parents had reported that many of these youth were showing a previously unusual pattern of symptoms. These adolescents seemed to be developing gender dysphoria without having shown any obvious gender-related distress earlier in their childhoods. Often, however, these adolescents had pre-existing mental health issues.
Littman coined the term ‘Rapid Onset Gender Dysphoria’ (ROGD) to describe this syndrome, because of parental reports of gender distress appearing ‘out of the blue’. However, there is no reason to believe that social influences always operate rapidly as opposed to over a longer period of time. As far back as 2019, Littman herself acknowledged that “The potential pathways of social influence and maladaptive coping mechanisms leading someone to interpret their feelings as gender dysphoria and to seek transition may ultimately be more relevant than the perceived rapidity of the onset” of ROGD.
Littman’s original study of ROGD, which was based on parental reports, found that two thirds of adolescents with perceived ROGD had at least one friend who came out as trans at a similar time. This suggested that peer influences might have played a role in their decision to transition.
While research into ROGD has been helpful in highlighting social influences on transition, unfortunately some people interpret this research as suggesting that gender clinic patients are either purely socially-influenced or ‘truly trans’ (and not socially influenced at all). As may be obvious from what I’ve already written, it seems more likely that social influences play a role in most, perhaps all, decisions to transition - just in different ways, and in combination with different factors. While gender clinic patients are far from homogenous, the social influence hypothesis does not require that these patients fall into completely distinct, easily identifiable ‘types’.
Testimonies from parents of trans-identified children, and from former members of the trans community, cast light on how peers might influence people towards transition. These sources report that within certain social circles, ‘being trans’ earns you respect, approval, and acceptance. This is particularly true in ‘woke’ online communities, as detransitioner Helena Kerschner writes:
On Tumblr, the situation was such that any claim to being “oppressed” would accumulate social credibility, while any unfortunate “privileged” status was justification for verbal abuse… It's understandable that any young person exposed to this kind of belief system would grow to deeply resent being white, “cis”, straight, or (biologically) male.
The beauty of gender ideology is it provides a way to game this system, so that you can get some of those targets off your back and enjoy the camaraderie of like-minded youths. You can’t change your race, pretending to have a different sexuality would be very uncomfortable in practice, but you can absolutely change your gender, and it’s as easy as putting a “she/they” in your bio. Instantly you are transformed from an oppressing, entitled, evil, bigoted, selfish, disgusting cishet white scum into a valid trans person who deserves celebration…
With the new pronouns often comes a wave of positive affirmation from friends and followers, and the subconscious picks up quickly that there’s a way to make the deal of being on Tumblr even sweeter.
This is the incentive I felt to comb through my thoughts and memories for things that might be further evidence that deep down, I wasn’t really a girl.
Peers and online trans influencers may also persuade young people that transition is the key to self-confidence and feeling good about themselves. Here’s how Ellie, a detransitioner who was interviewed by the BBC, explains the impact of online influencers on her decision to transition:
I watched some YouTube videos of trans guys who take testosterone, and they go from this shy lesbian to a handsome guy who is super-popular. I liked thinking of myself having that possibility - it felt like I should have a male body.
An example of someone who appears to fit the theme of a socially-influenced transition is Ollie Davies, a detransitioner who was interviewed by The Australian newspaper:
Ollie Davies was 26 years old and at the lowest ebb of his life when he made a decision to come out as a trans woman.
Suffering depression, anxiety and behavioural problems as well as a crisis of self-identity, he existed in what felt like a dissociative state. He had distanced himself from family. “I felt as if I had no free will,” Mr Davies says. “I was completely nihilistic and lonely and self-hating and had no self-esteem. I was experiencing a total loss of identity and lack of sense of self.”
Mr Davies, who was openly bisexual, had never questioned his gender identity as a child or young adult. But when people within his group of queer activist friends repeatedly suggested to him that he was trans, he began to believe it was true.
“Ultimately it came from suggestions from others, people just started suggesting that I question my gender,” Mr Davies said.
In addition to peer influences, influences from schools, the media, social media, and even some parents may also have fuelled the trans wave. For those whose gender distress is fuelled by these influences, a change of friend group, a long trip, and/or a break from the internet, may ease their distress.
Accepting gender identity theory
As a hypothesised psychological condition becomes better known, more people tend to start saying that they have it. This happens because people start to interpret their personal experiences through the lens of the condition. In some cases, such as electromagnetic hypersensitivity, believing in the condition can result in genuine symptoms that have no physical cause.
Something similar appears to have happened with trans identities. When people learn about the concepts of gender identity and gender dysphoria, some of them start to interpret their experiences through this lens. Emotional distress, trouble fitting in, and discomfort with the body or with sex stereotypes are all then perceived as signs of ‘being trans’.
This process then tends to build on itself in a self-reinforcing circle. For example, as a young woman immerses herself in gender identity theory, she learns that ‘misgendering’ (i.e. being called by the correct pronouns for her biological sex) is deeply harmful. This causes tremendous anxiety and distress, since inevitably most people around her will continue to (correctly) perceive her as female. In turn, she interprets this distress as a symptom of ‘being trans’, causing her to become more and more certain that she is ‘truly trans’.
An example of someone who seems to fit this theme is detransitioner Helena Kerschner. Helena has directly stated that “It was this weird belief system I found on the internet that made me want to be trans”, and that learning to doubt that belief system was a key part of her recovery.
The popularisation of gender identity theory (also known as gender ideology) in schools, social media, and the media may have contributed to the trans wave. Teaching alternate viewpoints may help resolve it.
Neurodiversity
There is a clear connection between trans identities and autism spectrum disorders (as well as other neurodiverse conditions). There are several plausible causes for this link. People with autism are often more rigid in their thinking, which could lead to the belief that if you don’t fit female stereotypes, then you can’t really be a girl (for example).
People with autism also frequently suffer from feelings of discomfort in their own bodies, which may be mistaken for symptoms of ‘being trans’. Additionally, the social difficulties that accompany autism may make people with autism especially susceptible to manipulative social influences. And the idea of medical transition as a cure-all is especially appealing to people on the spectrum, who often have difficult and socially isolated lives.
An example of someone who appears to fit this theme is a detransitioner called Ash, who when asked why he started identifying as transgender, says:
Well, I think one of the big parts was reading about the treatments and hormones and stuff. The biggest thing that made me attracted to it was... taking estrogen would cause facial hair and body hair to thin, and one of the things I've been struggling with... is having body and facial hair because it's a very unpleasant sensory experience for me and I hate the way it looks. I hate the way it feels and I hate the fact that if I want it to go away I have to shave it... but that's just life... I saw that at the time as a manifestation of gender, but I realize now that it's just something I do... that isn't a gendered thing.
It seems unlikely that neurodiverse conditions, by themselves, cause trans identities. Instead, neurodiverse conditions probably make people more vulnerable to the other causes that we’ve already discussed. Educating people with neurodiverse conditions about this vulnerability, and teaching them coping strategies, may help build their resilience to these influences.
Now that we’ve looked at the innate and social influence hypotheses in more detail, we can weigh the evidence for and against each of them.
Arguments for the innate hypothesis
I’ve searched extensively for arguments for the hypothesis that trans identities are innate and immune to social influences. I address the most common of these in the following sections.
Personal attacks on people with different views
Arguments for the innate hypothesis often consist chiefly of smearing anyone who disagrees with this hypothesis as “anti-trans”. One illustration of this is the essay ‘All the Evidence Against Transgender Social Contagion’, written by influential trans activist Julia Serano.
The very first item that Serano includes in his dot-pointed list of supposed “evidence” against the social influence hypothesis is not ‘evidence’ at all. This is the claim that “The concept of ‘transgender social contagion’ was invented by a trans-skeptical parent on February 2016 on the anti-trans website 4thWaveNow”.
Serano doesn’t really explain why he thinks this claim is evidence against the social influence hypothesis. Presumably, his aim is to discredit this hypothesis by implying that it was inspired by hostility towards transgender people. Possibly, he is suggesting that because social influences on transition were first noticed by a mere parent rather than a researcher or clinician, these observations are not ‘scientific’.
Of course, in reality it should not be surprising that parents would be among the first to notice a troubling new trend affecting their children. And parents’ doubts about permanently medicalising their children are simple common sense, not evidence of some nefarious “anti-trans” agenda.
In point of fact though, Serano appears to be mistaken about the origins of the social influence hypothesis. In 2015, researchers at a Finnish gender clinic published a peer reviewed paper expressing concern about an emerging cohort of adolescent patients whose profile was similar to what would later be described as “rapid onset gender dysphoria” (although they do not use this term). This paper was published before the blog post that Serano claims ‘invented’ the social influence hypothesis.
The Finnish research paper is based on clinical interviews and assessments of adolescents themselves, with input from their parents. The paper examines every adolescent who sought assessment for sex reassignment in Finland between 2011 and 2013.
The researchers note a sharp increase in referrals to their clinic, and describe a new group of patients for whom “medical [sex reassignment] treatments may not be currently advisable”. They note that “Adolescents are more suggestible and submit more readily to group pressure to gain acceptance”, and that some “might be prone to interpret a variety of their problems as being a result of gender incongruence, even if the problems actually were independent of gender identity issues”.
It thus seems that clinicians and parents started to raise concerns about the nature of the trans wave independently, around the same time, and based on similar observations.
Since the Finnish clinician-researchers specialised in providing medical care for trans-identified youth, it would stretch credulity to accuse them of being ‘anti-trans’. Nevertheless, no doubt some gender activists will attempt to do so. Since gender activists classify anyone who disagrees with the innate hypothesis as ‘anti-trans’ by definition, this type of name-calling is circular and unconvincing.
Ultimately, these sorts of personal attacks are neither interesting nor scientifically relevant. They provide no evidence for the innate hypothesis.
The left-handed analogy
A centrepiece of Serano’s argument is a chart (shown below) that he claims shows a “rise in left-handedness... as stigma against left-handedness receded”. This chart was originally sourced from the book ‘Right Hand, Left Hand’ by Chris McManus. As this book explains, the years shown in this chart refer to when the survey participants were born (not to when data was collected - Serano does not make this clear). The book also explains that the measured rate of left-handedness rises from about 3% among older participants, to about 12% among younger participants (not from 2% to 13% as claimed by Serano).
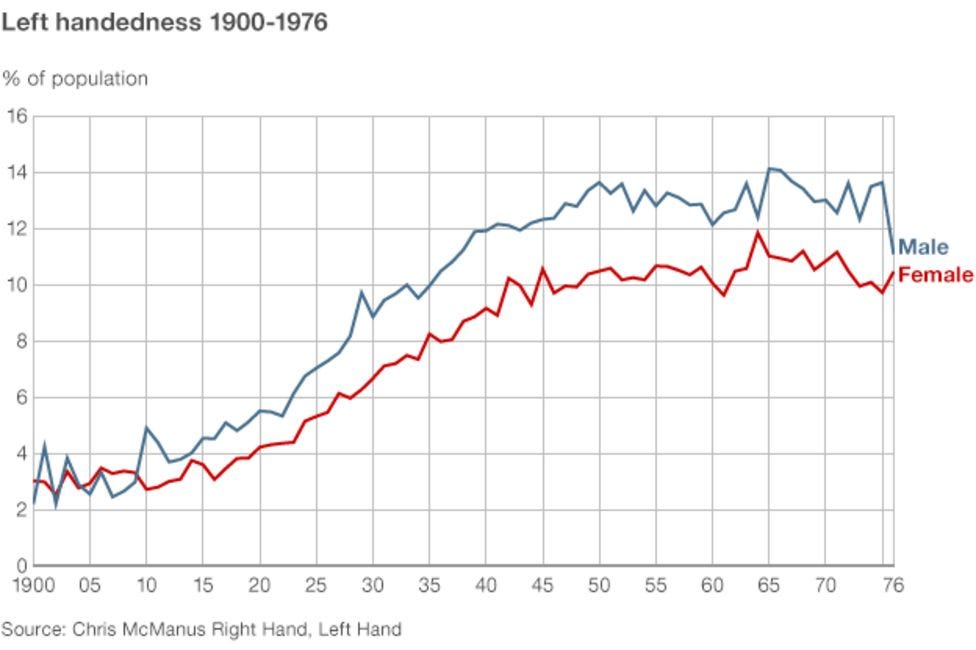
On the basis of this chart, Serano speculates that innate left-handers repressed their left-handedness during the 19th and early 20th centuries because of stigma. Serano goes on to speculate that innately trans people repressed their trans identities until recently because of a similar stigma. There are a couple of reasons this analogy is unconvincing.
First, there is no strong evidence that the rise in left-handedness was the direct result of reduced stigma. The causes of this rise are still uncertain. McManus himself (the author of the chart shown above) has argued that this rise was not directly due to reduced stigma, and was instead primarily caused by an increased frequency of the genes predisposing people to left-handedness. (Another seemingly plausible explanation for the rise of left-handedness is that schools gradually stopped forcing children to write with their right hand. However the survey controlled for this by asking respondents which hand they throw with, which is less likely to be affected by school instruction).
Second, and more importantly, there is no particular reason to believe that the causes of the trans wave are the same as the causes of increased left-handedness. There are many examples of behaviours that spread due to social influences, which seem more similar to the trans wave than does left-handedness (as I discuss later in this essay). The left-handed analogy thus fails to provide any real evidence that trans identity is innate.
Other authors have attempted to draw an analogy between trans identities and same sex attraction. I do think that same sex attraction is probably innate, but I don’t think that this proves that trans identities are innate. Consistent with this distinction, there is evidence that homosexual behaviour, but not gender dysphoria, was prevalent in the past and in traditional cultures (as shown later in this essay). I address this complex issue in greater depth here.
Evidence for genetic and brain differences
Some evidence suggests that on average, the brain morphology of transgender individuals differs from that of non-transgender people. This evidence is commonly cited in support of the idea that trans identities are innate.
However, there is an interesting quirk to these brain differences. There is evidence that homosexual (male-attracted) transwomen show a pattern of brain morphology which is, in certain regards, more female-typical than is usual among other men. This mirrors the findings for other homosexual men, who show a similar pattern. This is consistent with the social influence hypothesis, which proposes that homosexuality and gender non-conformity are risk factors for (but do not determine) a trans identity.
In contrast, heterosexual transwomen do not appear to show the pattern of ‘brain feminisation’ often seen in their homosexual counterparts. Instead, they (on average) show an unusual pattern of results, perhaps reflecting the neurodiversity that is a known risk factor for a trans identity (as proposed by the social influence hypothesis).
These two distinct brain scan patterns are incompatible with the favoured trans activist narrative, which suggests a single cause for transgenderism (i.e. having an innate, mismatched gender identity). If there was a single cause, we would expect a single pattern of brain differences, rather than two completely different patterns.
Research suggesting that trans identities are somewhat heritable can be explained in much the same way as trans brain differences. Both homosexuality and neurodiversity are partly genetic. Genes may lead directly to homosexuality or neurodiversity, and only indirectly to the development of a trans identity.
Finally, it remains to be seen whether the genetic and brain imaging differences discussed above will be found in the newer, adolescent-onset cohorts of socially-influenced transitioners - time will tell.
Overall then, these genetic and brain imaging findings provide little support for the innate hypothesis.
Trans testimonies
Of all the arguments for the innate hypothesis, perhaps the most emotionally powerful is the testimony of trans adults. It’s natural to be swayed by the emotive personal story of someone who claims that “I was born trans”. For example, this 2017 Guardian article tells the stories of several trans adults, some (but not all) of whom claim to have known that they were trans from a very young age. The article implies that the only explanation for this is that trans identities are innate.
The most obvious flaw in this logic is that the ‘born this way’ narrative does not fit everyone who identifies as trans. As we’ve already seen, many trans people’s stories are entirely consistent with the social influence hypothesis. In a recent Washington Post survey, 68% of transgender adults reported that they did not “begin to understand that [their] gender was different from the sex [they] were assigned at birth” until at least the age of 10, consistent with the possibility that their trans identities developed over time rather than being innate. Conversely, numerous adults have testified that they showed ‘classic signs’ of being transgender in childhood, but simply outgrew this phase.
Another serious flaw in this logic is that it relies entirely on unverified childhood memories. Childhood memories are known to be highly malleable, and prone to distortion and bias based on current beliefs and motivations. Since many trans adults are highly committed to the innate hypothesis, it is probable that they are prone to recall and interpret their childhood in ways that are consistent with this narrative. For example, emotional distress, social awkwardness, gender nonconformity, and/or a fondness for opposite-sex clothing may be recalled as if they were sure signs of ‘being trans’ (when other interpretations of these experiences are entirely plausible). It’s well known in psychology that introspection is not a reliable guide to the inner workings of our minds, and this is doubly true when relying on memories of the distant past.
Finally, as discussed earlier, the social influence hypothesis proposes that believing in gender identity theory is a risk factor for experiencing gender dysphoria. So it should be no surprise that many (although far from all) trans-identified individuals believe in gender identity theory.
For these reasons and more, trans testimonies fail to provide convincing evidence that trans identities are innate.
Gender clinician opinions
As we’ve seen, some clinicians who work with gender-distressed youth have endorsed the social influence hypothesis. Other clinicians deeply oppose it, and their opinions are sometimes held out as if they were strong evidence that social influence is not occurring. For example, this 2023 Scientific American article relies heavily on gender clinician opinions to support its claims.
It should be obvious that gender specialists have a strong financial, professional, and personal incentive to dismiss and discredit the social influence hypothesis. The thought that you may have spent years of your career damaging vulnerable children is no doubt too horrible to contemplate. And, to paraphrase Upton Sinclair, it’s difficult to persuade someone to believe something when their salary depends on them not believing it.
Nonetheless, the Scientific American article presents the gender clinicians it quotes as if they were disinterested scientific ‘experts’. In contrast, the article paints concerned parents as “anti-trans”, insinuating without evidence that they are deeply biased and motivated by bigotry rather than love for their own children. This double standard is perhaps unsurprising from Scientific American, which was once considered a credible information source, but has more recently been criticised for sacrificing scientific objectivity in favour of various activist causes.
Of course, just because gender clinicians are inevitably swayed by their financial and personal incentives, this doesn’t mean that they are deliberately harming their patients. Many clinicians have misplaced faith in the flawed guidelines written by activist/professional organisations like WPATH. Others simply take the say-so of their young patients as gospel. Diane Ehrensaft, one of the ‘experts’ quoted by Scientific American, makes this clear:
In some ways, [kids] are far more advanced than I am, as somebody in my 70s, about how they live and understand gender… So if we want to really understand gender, turn to the experts—and that would be the youth themselves.
It doesn’t appear to have occurred to Ehrensaft that her young patients’ beliefs about gender identity might have been picked up from YouTube, TikTok, school, and the playground; rather than reflecting the innate and infallible wisdom of youth.
Nor does Ehrensaft acknowledge that she herself could be influencing her patients’ beliefs about gender identity. Yet, because of their position of trust and authority, health practitioners have a potentially huge sway over vulnerable patients. When Noah, who we met earlier, was asked what made her feel safe to medically transition in her teens, she replied:
To me, what's important is that I had a team of medical professionals who had done this and who could help me make the right decision and helped guide me... I think what's crucial is that I was not the only person making these decisions for myself. I expressed how I was feeling to adults and to professionals. And they came to medical conclusions the same way you would about undergoing any sort of medical procedure.
In other words, gender clinicians believe that trans identities are innate because their patients tell them so. And gender clinic patients believe that trans identities are innate because gender clinicians (as well as YouTube influencers) tell them the same thing. It’s easy to see how this circular confirmation could lead both patients and their clinicians to become increasingly, but incorrectly, confident that they are innately trans.
Overconfident ‘expert clinical opinion’ has a long history of tragic error. There is every sign that gender clinicians’ beliefs about the origins of the trans wave fall into the same category.
Studies show…
Both Serano and the Scientific American article claim that specific studies have ‘proven’ that social influence on trans identities does not occur (thus implying that trans identities are innate). Some of the studies referred to by Serano do not in fact seem to directly address this question. Without getting into the weeds on those studies that do, suffice it to say that their flaws have been repeatedly and convincingly criticised. Both Serano and Scientific American, of course, fail to inform readers that these criticisms exist.
Evidence for the social influence hypothesis
Trans medical interventions do not reliably improve mental health
One of Julia Serano’s justifications for the innate hypothesis is the claim that medical gender transition improves youth mental health. He holds up this alleged improvement as evidence of patients’ innate transgender identities.
As mentioned earlier, the idea behind this claim is that everyone has a gender identity which may or may not match their biological sex. When gender identity mismatches appearance, a special type of distress (called gender dysphoria) is the result. Supposedly, the only solution to this distress is to use surgery and/or hormones to reshape the person’s appearance.
However, the effectiveness of medical transition has long been controversial, and it is now becoming increasingly clear that medical transition does not reliably improve youth mental health. The widespread belief that it does is probably due to placebo effects, combined with the influence of some hugely impactful but badly flawed early research. As I wrote last year:
As the British Medical Journal has reported, multiple systematic reviews have found scant evidence for the safety or effectiveness of youth transition. Researchers have found serious flaws in the studies often cited to justify these treatments.
As The Economist recently reported, “Until now, transitioning has been justified by the hope that it could ease distress. Though some studies have found short-term improvements in mental health, these disappear in long-term studies”. For example, a European 2021 study tracked 873 patients who started taking cross-sex hormones. Some subgroups of patients initially experienced a small lift in mood, possibly due to placebo effects. However, these benefits disappeared within three years of initiating treatment.
Similarly, the best evidence suggests that medical transition does not mitigate suicide risk. For example, a 2020 study examined suicide rates among 8,263 people who medically transitioned at the Amsterdam University Medical Centers. It found that “suicide deaths occurred during every stage of transitioning” and “the incidence for observed suicide deaths was almost equally distributed over the different stages of treatment”.
Social transition (i.e. treating someone as if they were the opposite sex) appears to be equally ineffective. Three high-quality studies have found that socially transitioning children has few if any mental health benefits.
There have also been numerous reports, by both parents and youth themselves, of cases where transition has led to a significant deterioration in mental health.
The supposed mental health benefits of transition were always one of the key arguments for the theory of an innate gender identity. The failure of these benefits to materialise casts serious doubt on this theory.
Levels of detransition are high and rising
As Serano points out, the social influence hypothesis suggests that the trans wave will “likely [lead] to greater levels of transition regret or detransition over time”. If more people are transitioning due to social influences, or in a misguided attempt to reduce general psychological distress, this would predict that their trans identities are likely to be less enduring than for past cohorts of people who have transitioned for other reasons.
Serano makes the dubious claim, supported by a few cherry-picked studies, that no such increase in detransition is occurring.
In reality, recent studies suggest that up to 30% of young people who take cross-sex hormones detransition within just a few years. This is a much higher rate than found by early studies. While those early studies had serious flaws, and more recent studies remain far from perfect, nonetheless the pattern of results across studies suggests that detransition rates are rising over time. This has occurred despite inadequate healthcare support for detransitioners, combined with intense social pressure within trans social circles not to detransition.
Consistent with the social influence hypothesis, research suggests that detransition is often prompted by the realisation that transition was not helpful. A study of 237 detransitioners found that the most common reason for detransitioning was realising that their gender dysphoria was related to other issues (70% of participants). Other common reasons were realising that transition did not help resolve their dysphoria (50%) and finding alternative ways to resolve their dysphoria (45%).
Detransitioners often recognise that they transitioned due to social influence
Research into young people who detransition (e.g. stop taking opposite sex hormones) suggests that they often recognise that their initial transition was prompted by social influences. This includes both a belief in gender identity theory, and influence from peers, teachers, and online influencers. Here’s an example of how one research participant explained the impact of gender identity theory on her decision to medically transition:
People said well, everyone has a gender identity. So, if… you're happy being a woman and you're happy being treated like a woman, then you have a female or a woman's gender identity or whatever. And I felt like Oh well, I'm not so I must be a man gender identity… So I felt like OK that's the path I have to go down… it was definitely being told… if you don't identify as a woman, then you're transgender.
She says that she eventually realised that the concept of gender identity is “just kind of nonsense”, and has now detransitioned.
Gender identity theory is often an integral theme in stories of transition and detransition (see this article for further examples). In fact, a recent study of 100 detransitioners found that the most common reason given for detransitioning was that “My personal definition of female or male changed and I became more comfortable identifying as my natal sex”.
Online and peer influences emerge as another key theme in research into detransitioners’ stories. The same recent study of 100 detransitioners found that:
Participants identified sources that encouraged them to believe transitioning would help them. Social media and online communities were the most frequently reported, including YouTube transition videos (48.0%), blogs (46.0%), Tumblr (45.0%), and online communities (43.0%)... Also common were people who the respondents knew offline such as therapists (37.0%); someone (28.0%) or a group of friends (27.0%) that they knew in-person... More than a third of the participants (37.4%) felt pressured to transition... Clinicians, partners, friends, and society were named as sources that applied pressure to transition, as seen in the following quotes: “My gender therapist acted like it [transition] was a panacea for everything;” “[My] [d]octor pushed drugs and surgery at every visit;” “I was dating a trans woman and she framed our relationship in a way that was contingent on my being trans;” “A couple of later trans friends kept insisting that I needed to stop delaying things;” “[My] best friend told me repeatedly that it [transition] was best for me;” “The forums and communities and internet friends;” “By the whole of society telling me I was wrong as a lesbian;” and “Everyone says that if you feel like a different gender…then you just are that gender and you should transition.”
This research suggests that social influences are a major reason that people transition. As the quotes above illustrate, these social influences do not merely reflect greater acceptance of pre-existing gender identities. Rather, young people are being actively encouraged, and sometimes even pressured, to consider transitioning.
The trans wave is linked to social influences and the spread of gender ideology
Social influences on transition are not limited to detransitioners, but are instead a broader phenomenon. For example, a large study has shown that media coverage of transgender issues tends to prompt a surge in referrals to gender clinics.
In schools too, teaching gender ideology seems linked to the spread of trans identities. I’ve written previously about one dramatic example of this:
In 2016, Pittsburgh Public Schools started training all its staff in concepts of gender identity. This initiative grew into a comprehensive “plan of building acceptance and understanding around concepts of gender identity and expression” among students, staff, and school families. Astonishingly, by late 2018 nearly one in ten students in this school district identified as transgender, genderqueer, nonbinary, or another unspecified gender identity; potentially putting them on a pathway towards lifelong medicalisation.
Peer and online influences are also associated with adolescents’ decisions to transition. A large survey of parents who perceived their children as having Rapid Onset Gender Dysphoria found that “60% of female and 38% of males adolescents had at least one friend who declared a transgender identity around the same time”, and that “Parents estimated that their children spent about 4.5 hours per day on the Internet and social media prior to the onset of gender dysphoria”.
While studies of socially-influenced transition are sometimes criticised for over-relying on parental reports, parent surveys are a standard and well-accepted research method in child psychology. The results of parent surveys are also consistent with observations by at least some clinicians. For example, Dr. Riittakerttu Kaltiala, chief psychiatrist in the department of adolescent psychiatry at Tampere University Hospital, describes the pattern her team observed in Finland:
Around 2015… a new set of patients started arriving at our clinic. We began to see groups of teenage girls, also usually from 15 to 17 years of age from the same small towns, or even the same schools, telling the same life stories and the same anecdotes about their childhoods, including their sudden realization that they were transgender—despite no prior history of dysphoria. We realized they were networking and exchanging information about how to talk to us. And so, we got our first experience of social contagion–linked gender dysphoria.
Additionally, as we’ve seen, the results of parental observations are consistent with reports from formerly transgender adolescents (i.e. detransitioners). And moreover, when we listen carefully to currently trans-identified youth, their stories often reveal the same peer and online influences reported in parent surveys. One trans-identified child tells her story in a local New Zealand newspaper, in an enthusiastic article titled ‘Rainbow club reaches new heights’. She is charmingly open about the reasons she adopted a trans identity:
I’m Jay and I’d like to tell you a bit about myself before I start telling you about my story. I’m a year 9 at Whakatāne High School, I’m 12 years old and transgender.
It all started December of 2020. I was influenced by a fellow friend of mine named Theo, who is also transgender.
He was a really nice and cool person to hang out with, but he gave me huge gender envy, so I started dressing more masculine at home and using all pronouns to just see what I’m most comfortable with... January of 2021, I came out as trans and used the name Jayden at the time.
Noah, who we met earlier, volunteered to be interviewed on a podcast so that she could prove that young people were definitely not being socially influenced into transition. Nonetheless, she acknowledges that spending an astonishing amount of time watching trans-themed videos played a key role in her “gender journey” (i.e. surgically removing her breasts). Here’s Noah:
I watched every TED talk about every remotely queer subject that there was... When I was in middle school, I started discovering portions of the internet where people would talk about queer identity issues... My sort of gateway was Buzzfeed because they have a ton of viral content... Jammi Dodger, whose video was titled Dear Buzzfeed or something similar... I must have watched that 20 times.
From Buzzfeed, I started doing my own research when I was 11. I used to just rewatch videos over and over of trans men documenting their journeys online. And even before I understood why I was fascinated with that content, that's just all I would do is just rewatch videos like that. And I took all of that information in and I came to the conclusion I should allow myself to explore who I am and try and use that as an avenue to find happiness.
Similarly, in an ‘educational’ video targeted at school children, a New Zealand soap opera star acknowledges that consuming online trans content was a key part of her decision to transition:
So I think I was about 14 when I first started playing around with my gender. Obviously there’s been moments in my life before then that have been, kind of, not strictly male or female. And I felt quite comfortable flipping between the two. But I think it was when I hit school and worked out that girls do this and boys do that, and it started not working for me. So, I think God bless the internet is all I’m going to say because that really gave me the resources and the curiosity to go and look at what’s out there, and that gave me a lot of strength to pursue finding out who I really am.
The connection between social media, online influences, and the spread of trans identities has become so conspicuous that it is acknowledged even by trans-activist-friendly outlets like the New York Times, who write frankly that:
Social media has been a significant catalyst for teenagers questioning their gender identities today.
“I think a big part of it is definitely the internet,” said Indigo Giles, a 20-year-old college student in Austin... Mx. Giles said they realized they were nonbinary after finding a community of like-minded people on Tumblr. “People who have maybe been having these feelings for a long time, but haven’t had the words to put to them, finally can see, in such a readily accessible way, others that feel the same,” they said.
While the NYT article claims that social and online influences merely support kids to disclose pre-existing trans identities, this claim does not stand up to scrutiny. It does not explain why clusters of cases occur in particular schools and small towns, nor the experiences reported by detransitioners.
Moreover, a close look at the actual materials that can be found online, in schools, in libraries, and on social media shows that they teach toxic and misleading ideas about ‘gender’. These materials teach kids to misinterpret emotional distress, trouble fitting in, and discomfort with traditional gender roles and with their developing bodies as signs of ‘being trans’. And they implicitly promise that gender transition leads to confidence, social acceptance, and true happiness.
As we’ve seen, these messages are pushing young people towards decisions that often fail to provide the benefits they are hoping for, and that they may later regret.
Trans identities are often temporary
One reason to believe that left-handedness is innate is that it is typically stable over time. Trans identities, on the other hand, are often not.
Instead, research suggests that when young people experience gender distress, it often resolves naturally over time. Britain’s National Health Service has warned that among “children and young people”, gender distress “may be a transient phase”. Extended clinical assessment has shown promise in identifying gender clinic patients whose trans identity is unlikely to endure for long. And as we’ve already seen, high rates of detransition demonstrate that even in adulthood, trans identities are frequently unstable.
There are also people who declare themselves to be ‘gender fluid’, and report that their gender identity can change from day to day.
All this is very hard to reconcile with the idea that trans identities are innate. If gender identity can change, it must change because of something. And social influence is likely to be one such causal factor.
The size of the trans wave is too large for acceptance alone to plausibly explain
Until recently, medical gender transition was extremely rare. In 1955, the influential sexologist Alfred Kinsey attempted to track down every transsexual (as they were then called) in the United States. Kinsey has been widely criticised for overstating the prevalence of unconventional sexual variations, but even he was unable to locate more than a handful of transwomen and two transmen in the entire country.
In the late 20th century, more systematic international research likewise found very low rates of gender transition. This research found that about 0.15 people per 100,000 population initiated treatment for gender issues each year (most of these were natal males). We can compare this to data showing that in 2018, roughly 42 per 100,000 people in Wellington (New Zealand’s capital city) initiated similar treatments, a rate 275 times as high. Similar dramatic increases have been seen in the United States and around the western world, and have especially affected girls and young women.
It could be argued that perhaps if medical transition had been more readily available in the past, it would have been sought out more often. To evaluate this possibility, we would ideally like to know how many people identified as transgender, and/or suffered from gender dysphoria (and thus would have been potential candidates for medical transition). When searching for relevant historical evidence though, it’s crucial to remember that gender nonconformity (which has probably existed throughout history) does not imply a yearning to transition. As such, it is not, in itself, indicative of either gender dysphoria or a transgender identity.
To my knowledge, the highest quality surveys of gender dysphoria in the 20th century were two structured interview studies conducted in Iceland and Taiwan in the 1980s. The Icelandic researchers interviewed 862 randomly selected adults between March 1987 and March 1988. They did not find a single case of transsexualism (the diagnostic term then used to describe gender dysphoria). Only one person reported prior gender dysphoria, which had almost certainly resolved without medical intervention (which was not available in Iceland at the time).
The Taiwanese researchers interviewed eleven thousand randomly selected adults between 1982 and 1986. Their results suggested that only 0.02% of the Taiwanese population suffered from gender dysphoria at that time. Their results also suggested that a further 0.04% of the population had previously suffered from gender dysphoria which had since resolved.
In summary, both the Icelandic and Taiwanese studies indicate that until quite recently, gender-related distress was extremely rare in adulthood.
While childhood gender dysphoria was also considered rare in the 20th century, unfortunately this observation does not appear to have been quantified by high quality surveys. However, the Icelandic and Taiwanese studies help cast light on this matter. When children experience gender dysphoria, either it resolves over time, or the children grow into adults with gender dysphoria. Thus, the fact that adult gender dysphoria was very rare in the 20th century indicates either that childhood gender dysphoria was also very rare, or that it almost always resolved naturally before adulthood, or both. This is exactly what clinicians observed at the time.
It’s true that a few children did experience gender dysphoria even before our recent cultural shifts. For example, the endocrinologist Harry Benjamin (a famous pioneer of medical gender transition) reportedly received a few letters from teenage children requesting cross-sex hormones. However, claims that ‘trans kids are not new’ ignore the evidence that until recently, childhood gender dysphoria was a very rare, mostly temporary condition. These claims are thus highly misleading.
Another way of quantifying the trans wave is to compare the rates of trans identities among young people to rates among older adults, who have been less affected by the trans wave. Because at least some older adults have presumably been influenced by recent social trends, this almost certainly produces an overestimate of past rates of trans identities.
A recent Pew Research survey found that an astonishing 5.1% of US adults under 30 identify as trans or non-binary. This compares with 0.3% of adults over 50, and a rate of gender dysphoria of about 0.02% in the 20th century studies. So, the current rate of trans identification among young adults is 17 times higher than among older adults. And it’s over 200 times as common as gender dysphoria was in the 20th century.
In some places, current rates of trans identification are even higher. As mentioned earlier, a study of one US school district found that nearly one in ten students identified as trans or non-binary (over 30 times the rate that Pew found for older adults, and hundreds of times the rate of gender dysphoria found by the 20th century studies).
It is difficult for ‘greater acceptance’ alone to explain these dramatic changes. For example, the 5.1% of young US adults who identify as trans or non-binary compares with about 1.6% in New Zealand. ‘Greater acceptance’ can only explain this difference if Americans are three times as accepting of trans people as New Zealanders. In reality, survey data show that Kiwis are significantly more accepting of trans people than their US counterparts. A more plausible explanation for this difference is that the widespread promotion of gender ideology started earlier in the US than in New Zealand.
Another serious problem for the innate hypothesis is the lack of evidence for ‘hidden’ trans identities in the past. The innate hypothesis implies that throughout the 20th century, a huge number of people were secretly trans (at least 5% to 10% of the population, based on the current prevalence studies mentioned above). The innate hypothesis also implies that these individuals must have been fostering a hidden but obsessive longing to socially and medically transition, which would have led to widespread misery. It is simply not credible that such a longing would not have been extensively recorded in art, literature, personal diaries, and suicide notes from those unenlightened former times. Presumably it would also have shown up in the interview-based studies mentioned above (in the same way that research found ample evidence of homosexual behaviour in the same era). It’s very unlikely that large numbers of people were hiding trans identities in the 20th century (unless trans identities can be suppressed without incurring much distress).
Of course, it’s impossible to completely disprove the possibility that in the 1960s, 10% of the population were made miserable by suppressed trans identities, but for some reason never showed any outward sign of their suffering. Analogously, there is no way to completely disprove the possibility that a china teapot is secretly orbiting the sun, or that there are leprechauns hiding in my garden. Until we see solid evidence to support the claim that trans identities have ‘always existed’ in similar numbers to today, there is no reason to believe it.
Finally, trans activists have failed to present any credible rationale for why 5% to 10% of the population would have an innate predisposition to long for medical transition. Julia Serano, for example, simply claims that trans identities are part of “natural variation” that “for reasons inexplicable to everyone involved (including us!)… just randomly spring up”.
From a scientific perspective, this lack of a credible evolutionary basis for innate trans identities is highly unsatisfactory. In the environment we evolved in, medical transition was simply not an option, so a disabling longing to transform your body to look like the other sex would have been very bad for survival and reproduction. Disabling conditions do occur as part of natural variation, but evolution typically restricts them to low rates of occurrence, at least among the young.
In conclusion, evidence suggests that until recently, it was very rare for people to identify as trans, experience gender dysphoria, or want to medically transition. When gender dysphoria did occur, it usually resolved naturally over time. This evidence suggests that the trans wave is something genuinely new, rather than the unveiling of a phenomenon that has always existed. Social influences are the only plausible cause of this dramatic societal change.
Traditional cultures rarely produce people who want to medically transition
A common activist claim in support of innate trans identities is that transgender people exist in traditional cultures. The examples most commonly given include the fa'afafine of Samoa and the muxe of southern Mexico. However, researchers who have worked closely with these groups dispute that they map neatly onto the transgender phenomenon.
As psychology professor Paul Vasey writes in Newsweek:
In both places, I work with individuals who are male, but who present a markedly feminine manner. For example, many wear female-typical clothing and adopt feminine names…
Having interviewed hundreds of such individuals, I can tell you that almost without exception they are exclusively attracted to masculine men as sexual partners…
But Westerners err when they call these individuals "trans women," because the vast majority of fa'afafine and muxes actively reject being labeled as women…
Unlike many trans people in the West who identify as male-to-female, fa'afafine and muxes recognize that they have male bodies and that these are immutable. A tiny number might femininize their bodies with hormones or even more rarely surgery, but no one in their local communities, least of all fa'afafine and muxes themselves, believe that such procedures transform them into females. Given that they do not identify as women and recognize that they are male, dysphoria about sex or gender has traditionally been relatively uncommon in these cultures, my research has shown.
This cross-cultural research supports the idea that both same-sex attraction and gender non-conformity are innate and part of natural variation (given that they commonly occur in other cultures). However, the concept of innately trans individuals who need to be treated as if they were truly the opposite sex, and who need to medically transition to be happy, appears to be a recently invented Western idea.
The trans wave has occurred in concert with deteriorating youth mental health
The trans activist narrative proposes that:
The recent spike in trans identities and medical transition is due to increasing societal acceptance.
The poor mental health experienced by trans people is due to a lack of societal acceptance (i.e. “minority stress”).
The trans activist narrative thus predicts that, since societal acceptance has been increasing, transgender mental health should have been improving. More generally, this narrative predicts that people in general should be happier, especially young people, since we now live in a more accepting world that allows young people to be their true selves and flourish.
The social influence hypothesis, in contrast, suggests that the drivers of the trans wave are less positive. For example, this hypothesis suggests that increasing numbers of youth are transitioning in a misguided attempt to alleviate psychological distress. Additionally, the rise of social media may have contributed to both increased rates of transition and deteriorating mental health. Social messages that destabilise young people’s identities may have had similar effects. The social influence hypothesis thus predicts that, in general, increasing rates of transition will be associated with worse youth mental health.
The data are consistent with the social influence hypothesis. As rates of trans identification and medical transition have soared, so too has youth psychological distress. Increased symptoms of anxiety and depression have been seen in young people overall, LGBT individuals as a group, and trans-identified youth in particular.
The chart below illustrates this trend. It shows the association between increasing rates of medical gender transition and increased rates of psychological distress among New Zealand youth. As I wrote in 2022:
As the chart shows, the trans wave has happened in concert with a tripling in rates of youth psychological distress. This evidence is hard to reconcile with the belief that the social influences causing increased transition are entirely beneficial.

Evidence suggests that this deterioration in youth mental health is real (i.e. it’s not just that young people are reporting their problems more candidly). Sadly, rising youth psychological distress is reflected in increased rates of self harm.
Another piece of evidence comes from looking at age differences. As we’ve already seen, older generations have been much less caught up in the trans wave than young people. The gender activist explanation for this is that younger people have stopped repressing their innate true selves, allowing them to flourish. In contrast, older people are supposedly still repressing their true selves and suffering as a result.
If this story was correct, we would expect youth mental health to have improved relative to that of older people. In reality however, the opposite has occurred. Youth mental health has declined sharply, while that of older people has stayed relatively constant. Again, this is consistent with a connection between the trans wave and deteriorating youth mental health.
Emotional distress appears to precipitate transition
As discussed earlier, increasing numbers of young people appear to be transitioning because they believe it will alleviate general psychological distress. For example, in the recent study of 100 detransitioners mentioned earlier, 71% stated that they transitioned because “I thought transitioning was my only option to feel better”.
Studies of gender clinic patients further support the idea that emotional distress may precipitate transition. An article in the Telegraph aptly summarises the psychological state of the patients attending the Tavistock Gender Identity Development Service (Gids) in London:
Less than two per cent of children in the UK are thought to have an autism spectrum disorder, but according to Gids’s own data, around 35 per cent of its referrals “present with moderate to severe autistic traits”.
In 2000, the only clinical audit of patients ever carried out by Gids found that more than 25 per cent of referrals had spent time in care, compared with 0.67 percent of the general population. Children referred to Gids were ten times more likely than the national average to have a registered sex offender as a parent, while 42 per cent had lost a parent through death or separation, and 70 per cent had more than five “associated features” such as anxiety, depression, abuse, self-harm, bullying, eating disorders or suicide attempts.
Anna Hutchinson, a former Gids clinician who was interviewed for the book, “feared she may be contributing to a medical scandal, where an NHS service was not stopping to think what else might be going on for so many of these vulnerable children”, the author notes. Only 2.5 per cent of the children seen at the clinic had no associated problems.
Gender activists often attribute the poor mental health of trans-identified children to ‘minority stress’, that is, a lack of societal acceptance. This seems to contradict the argument that these children are transitioning due to increased societal acceptance. Moreover, childhood mental health problems often precede trans identification, making lack of societal acceptance an unlikely explanation. And since gender transition often fails to resolve these problems, ‘repressed trans identities’ are not a convincing explanation either.
Most tellingly, ‘minority stress’ cannot explain why so many of these children had lost parents to death or separation, nor why so many had sex offenders as parents. Nor is it plausible that ‘minority stress’ causes autism, which is widely accepted to have genetic and biological causes. Rather, it seems far more plausible that these risk factors make children more vulnerable to identifying as trans.
The trans wave resembles other socially-influenced conditions
As mentioned earlier, many aspects of the trans wave are strikingly similar to the ‘repressed memories’ scandal. Eminent social psychologist Carol Tavris, writing in Skeptic magazine, has described many of these similarities. Therapist Lisa Marchiano has described others. In both recovered memory therapy and gender affirming therapy:
Many patients are psychologically distressed adolescent girls and young women.
Patients are taught by a trusted authority figure that they can uncover a previously hidden aspect of themselves (i.e. repressed memories, their ‘real’ gender identity). They are promised that this will help them to understand and resolve their longstanding psychological distress.
Patients are taught to reinterpret various aspects of their psychological distress as symptoms of an underlying condition (i.e. repressed memories, gender dysphoria).
Treatment outcomes are often disappointing, and some patients deteriorate during treatment.
Feelings, thoughts, and perceptions indicating that someone has the condition are held to be unerringly accurate (e.g. “The memories come from our body which doesn’t lie”, “Trans people are who they say they are”). Feelings of doubt, however, are dismissed as unreliable (“The doubts are not real... the memories are”, or “Only trans people are worried about if they are actually transgender!”).
Patients are taught that anyone questioning their recovered memories/gender identity is attacking them as a person.
Patients are taught that anyone sceptical of the movement is a bad person (i.e. an enabler of abuse; anti-trans; transphobic). They are encouraged to cut off contact with such people, even family members.
Patients are encouraged to become deeply immersed in movement content (e.g. books about sexual abuse; online trans influencer content) and social groups (e.g. survivor support groups, online trans forums, trans support groups).
Fellow group members reinforce ‘progress’ (recovering more vivid memories, transitioning gender) with enthusiasm, warmth, praise, and affirmation.
Both movements attached themselves to popular, genuinely valuable social causes (the campaign against child sexual abuse; the campaign for gay rights). Both movements have used these associations to camouflage their true nature, deflect criticism,and smear their critics.
The mainstream media and popular culture have played an important role in promoting both movements.
These commonalities are not random. Both movements apply a powerful system of influencing techniques that create new beliefs in vulnerable people. They achieve this by promising the patient a compelling reward, surrounding them with like-minded individuals, isolating them from alternative viewpoints, reinforcing ‘progress’ towards consolidating the new belief, and teaching patients to interpret challenges to the belief system as a personal threat.
The process of resistance to these movements has also played out similarly. In both cases, well-qualified sceptics were initially attacked or ignored, but persisted and gradually gained ground. The voices of ex-believers (retractors, detransitioners) were also initially dismissed, but became increasingly difficult to ignore.
Another condition with a striking resemblance to the trans wave is socially-induced tic disorder, popularly known as the ‘TikTok tics’. Tics are sudden, seemingly uncontrollable twitches or vocalisations. Most tics are believed to have a neurological origin.
In 2022, several clinics observed a sudden surge in patients presenting with tic disorder. Often, these patients’ symptoms bore an obvious resemblance to those of prominent ‘tic influencers’ on TikTok. Many of these patients were emotionally distressed adolescent girls who consumed large amounts of ‘mental health’ content online.
It seems very clear that the ‘TikTok tics’ are socially influenced, rather than neurological in origin. And it’s not just that they affect the same type of person as the trans wave, or that they spread in a similar manner (as this video by trans YouTuber Blaire White shows vividly). In many cases, the same people who are affected by socially-influenced tics also identify as trans. As the New York Times reports, a study of patients with the TikTok tics found that 43% were trans or non-binary. This finding suggests that both conditions may share a common origin: a socially-influenced response to psychological distress.
As various authors have pointed out, other socially-influenced behaviours that appear to spread in similar ways to the trans wave include transracialism, multiple personality disorder, anorexia nervosa, and self harm.
The trans demographic shift is consistent with the social influence hypothesis
One of the earliest pieces of evidence that caused concern about the trans wave was the trans demographic shift. In essence, the new cohort of young people seeking medical transition reflects the demographic profile of people who are vulnerable to peer influences and self-destructive social trends. As Antony Latham, a retired GP and the chair of the The Scottish Council on Human Bioethics, writes in a peer reviewed paper:
It might be argued that the increase in children presenting with [gender dysphoria] is due to the openness of society and the access to websites and advice that now exists. In other words, [gender dysphoria] in these numbers always existed but was repressed. This however is extremely unlikely for the following reasons:
The recent increase in [gender dysphoria] is almost confined to children approaching puberty and adolescence and, as we have seen, is usually rapid in onset. We would expect other age groups to be also presenting in greatly increased numbers if acceptability and access to help was the reason.
The belief that this is a new category of [gender dysphoria] is supported by the fact that a decade ago most [gender dysphoria] in children presented in early childhood. The numbers are so much increased around puberty years that it seems likely (though not proven), that this is a new phenomenon, rather than a consequence of historical repression.
The vast majority of new onset [gender dysphoria] occurs in girls. We know from previous data that gender dysphoria was more common in boys... This increase in girls parallels the considerable increase in anorexia nervosa in girls over the past decades..., and in self-harm among girls... suggesting a common underlying cause.
Beware selective demands for rigour
Like many other questions in medicine and the social sciences, identifying the causes of the trans wave is a complex challenge. It is not the type of question that can be conclusively answered by conducting a particular experiment, because of practical and ethical constraints. Rather, it is the type of question where knowledge is advanced by exploring patterns and correlations, and attempting to find the explanation that best explains these observations.
As such, evidence supporting one hypothesis or another will never be completely definitive. For example, the close similarities between the trans wave and the false memory scandal could be merely coincidental. Similarly, the sharp deterioration in youth mental health that occurred in concert with the trans wave could be coincidental as well. Given sufficient imagination, it will usually be possible to devise some potentially possible (if unlikely) alternative explanation for any piece of evidence that might bear on this issue. All we can say is that, when we consider multiple strands of evidence, such alternative explanations are highly implausible.
Where gender activists err is in justifying their own positions based on poor-quality or non-existent evidence, and yet holding others to impossible standards of scientific rigour. For example, systematic reviews have shown that youth gender medicine is based on very low quality evidence. Given the obvious risks involved, anyone truly committed to scientific rigour would support a pause on youth gender transition until long-term randomised controlled trials have been conducted (similar to the policies of several European countries). However, gender activists actively oppose such trials, perhaps recognising that the outcomes are unlikely to be favourable to their cause.
More broadly, gender activists have tried to suppress research and theoretical models that might cast light on the origins and impacts of the trans wave. Such further research and open debate is badly needed, and should be supported by anyone who genuinely cares about the wellbeing of gender questioning youth.
We need a more careful approach to youth gender medicine
In summary, there is no convincing evidence that gender identities are innate or immune to social influences. And there are multiple strands of evidence that, taken as a whole, strongly suggest that social influences have played an important role in encouraging more people to identify as trans, and to subsequently transition. These influences do not necessarily operate at a conscious level, and from an individual perspective, it may feel like trans identities are innate. But the evidence is clear.
Most parents do not want to see their children influenced into needless, lifelong medical dependency. Yet, incredibly, some trans activists claim that the trans wave has not had any “serious negative ramifications”. This shows a stunningly callous disregard for the immense damage that their ideology is doing to the health and happiness of a generation of young people. As Scott Newgent, a transman and stalwart opponent of youth medical transition, explains:
Anyone going through [medical transition] is in store for a brutal process… During my own transition, I had seven surgeries. I also had a massive pulmonary embolism, a helicopter life-flight ride, an emergency ambulance ride, a stress-induced heart attack, sepsis, a 17-month recurring infection due to using the wrong skin during a (failed) phalloplasty, 16 rounds of antibiotics, three weeks of daily IV antibiotics, the loss of all my hair, (only partially successful) arm reconstructive surgery, permanent lung and heart damage, a cut bladder, insomnia-induced hallucinations—oh and frequent loss of consciousness due to pain from the hair on the inside of my urethra. All this led to a form of PTSD that made me a prisoner in my apartment for a year.
Despite this immense suffering, for a long time Scott continued to believe that medical transition had been “the right path for me to choose”. But more recently, Scott has described medical transition as “[my] single most significant regret… one that never releases its grip”. Scott writes:
For me, gender transition was and continues to be dangerous, causing massive and recurring health issues. It cured nothing… I’m trans and I cannot detransition, even though I’d like to. The process has gone too far; there is no turning back.
This essay began by telling Sinead’s mother’s story, and how she believes that she saved her young daughter from the permanent medical damage suffered by people like Scott. Sinead’s mother was confident that she had done the right thing. I hope this essay gives other parents in the same position the confidence that they, too, are doing the right thing. The evidence is with you.
So thorough, so well written. Thank you. I wish everyone I know who’s been sucked into thinking that there’s nothing wrong with so-called “gender-affirming care” or “social transition” for children and teenagers would read this.
The easiest way to say it is that there's no such thing as "trans."
There is untreated mental illness. There is pornography and social media addiction. There is autogynephilia.
But nobody "transitions" sex and nobody is in the wrong body.